Week 4 & 5
Greetings from snowy Coeur d'Alene, ID!
I am so sorry for my late blog post! I have been traveling a lot these past two weeks and working at my internship, so it's been hard to write this post but here I am! This week I started my internship at CDA Spine and so far it has been such a cool experience shadowing Dr. Larson, working with x-ray technicians, and gathering the data for my research project.
On Monday, I learned how to use the Surgimap software, which is a computer program that allows researchers to take spinal parameter measurements from patient x-rays. Surgimap is an extremely helpful tool because it allows doctors and researchers to easily find a patient's Sacral Slope, Pelvic Incidence, Pelvic Tilt, Lumbar Lordosis, Thoracic Kyphosis, Sagittal Vertebral Axis, and Cobb Angle! Without this software, these parameters would be much more complicated to take. Moreover, the aforementioned measurements above are crucial to understanding the health of a patient's spine, especially if the patient is undergoing surgery. These angles allow the surgeon to make decisions on how to better correct or mend the spine to a desirable state for the patient's pathology.
To measure lordosis using the Surgimap software, you can use the Cobb measuring instrument or the Lumbar Lordosis measuring instrument. The only difference between the two is that the Cobb measurement will create a positive value and the Lumbar Lordosis measurement will create a negative value. I used the Cobb method because that was the way I was taught!

(You can't really see the instrument options in the tool bar, but I'd use the very first option, >Cobb. For some reason this picture doesn't show the pelvic incidence tool.)
For the purposes of my research, I needed to measure my research subjects' preoperative, post operative, and most recent global lordosis (L1-S1) and preoperative and postoperative segmental lordosis (the level where they received their one-level fusion). For example, if a patient received a MIS TLIF to remove a degenerative disc between the L4-L5 vertebrae, I would measure the preoperative to postoperative change in lordosis for the L4-L5 vertebral segments. In addition to measuring lordosis, I would measure a patient's pelvic incidence and pelvic tilt if both of the hips were visible in the x-ray. However, it was really rare to find a preoperative and postoperative x-ray with both hips. Even if a patient had a preoperative and postoperative x-ray with both hips the pelvic incidence, which is supposed to be a constant value for each patient, would change! The x-ray technician that I worked with said that even if you align both of the circles with the hips and the straight line with the endplates of the S1 vertebra like you did in the first x-ray (the preoperative x-ray), you can still get different measurements! Measuring pelvic incidence and pelvic tilt were by far the most challenging for this reason; also, it was hard to tell if the circles in the x-ray were gas bubbles or actually the hips! (I'll post some pictures later in this post to show you what I am talking about.) There was one time where I measured a pre-op and post-op pelvic incidence and the values came out to be the same. I was very proud!
Image of Global Lordosis (L1-S1)

Initially, I found the program to be complex because I was not familiar with reading x-rays and understanding where to draw the lines along the endplates — sometimes the imaging of the x-ray made it even more difficult to find the endplates of the vertebra. There were times where I would just have to make my best guess! The x-ray technician I was working with advised me to be consistent with the method I chose to use because there are a variety of ways to take these measurements. (It is all very subjective and arbitrary.) Eventually, I gained confidence in my method. I decided to draw the lines from the front endplate to the back endplate of the vertebra.
Taking this data was time consuming! It took me three six-hour work days to get measurements for 95 patients!
Here are some pictures I took of my data to give you a better idea! (FYI, patient names were removed for confidentiality reasons, but I will randomly make-up a name for the purposes of explaining...and because it’s fun!)
Extra: Here is a picture of an x-ray I measured with pelvic incidence and pelvic tilt

Extra: Here is a picture of an x-ray I measured with pelvic incidence and pelvic tilt

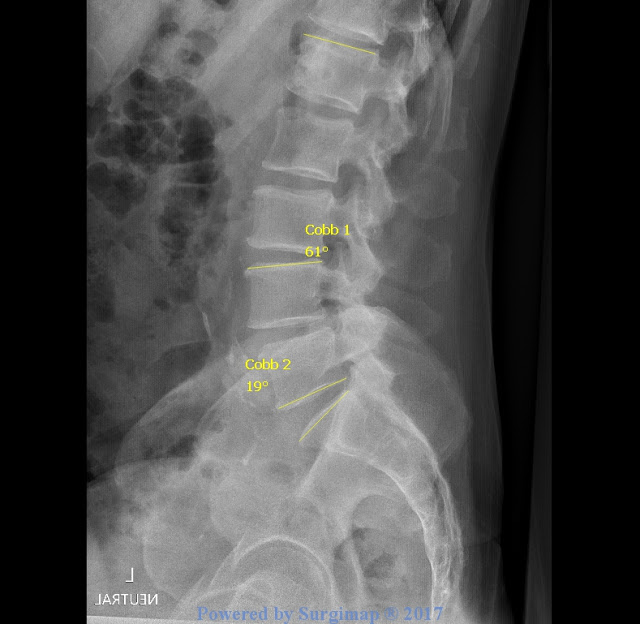
This here is Bob's preoperative x-ray. The segment where the surgery will be performed is the L4-L5 segment (indicated by Cobb 2). His global lordosis is 61 degrees and his segmental lordosis is 19 degrees. Remember, the aim of my research is to see what effects (if any) MIS TLIF has on global and segmental lordosis.
Bob L4-L5 Lumbar Fusion: Preoperative Image
This is Bob's six-week postoperative x-ray. His global lordosis increased 5 degrees and his segmental increased 3 degrees. While Bob’s global and segmental lordosis increased, we must remember that he is one subject and that his "trend" is not applicable to my larger population — at least not yet. When I was taking these measurements, it was hard to generalize a trend with pre-op and post-op change, which is why I will have to perform a two-tailed t-test to test the significance of the pre-op to post-op lordotic change.
Bob L4-L5 Lumbar Fusion: Postoperative Image
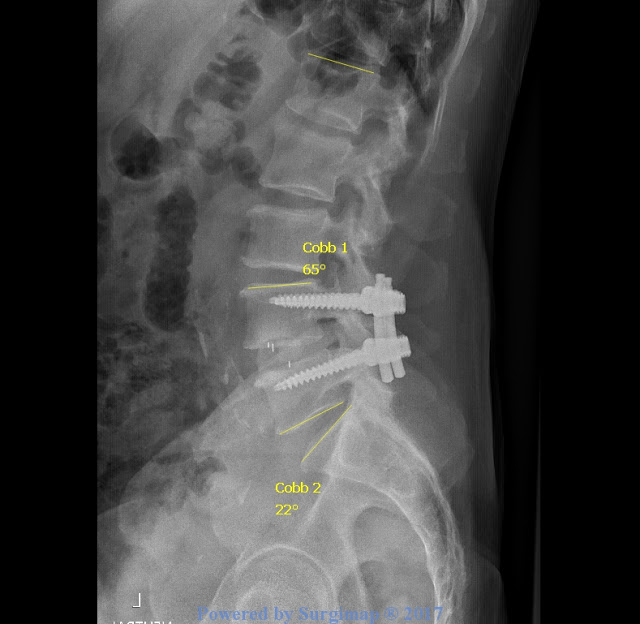
The three white lines in the disc space illustrate a traditional TLIF cage. There are two different cage types in my study: a TLIF cage and a PLIF cage. The TLIF cage is shaped like a pear, made from polyetheretherketone (PEEK), and has five degrees of inherent lordosis. In my study, TLIF cages were more prevalent in patients who received a MIS TLIF from 2012 to 2014. Bob must have been a patient during that time period because he received a TLIF cage. The PLIF cage that Dr. Larson uses looks like an elongated oval and is made of Tritanium. The PLIF cage has 6 degrees of inherent lordosis. (In my next blog post, I will further elaborate on the different cage types and their relevance to my study.)
Here is a picture of an x-ray with the PLIF Cage:

Here are two pictures of the sample PLIF cage used in my study: (the sample is MUCH bigger than the actual cage used in surgery.)


In addition to taking measurements, I got to shadow Dr. Larson around in clinic. Before Dr. Larson and I made our way to the exam rooms, Dr. Larson would show me the patient’s MRI and where the lumbar fusion was performed on the spine. Most of the patients I saw had already received surgery and were there for a post-op or one year check-up. For example, the first patient I observed had a L4-L5 fusion back in the fall and, for the most part, seemed to be in good spirits. Patient 1 complained about leg tingling and numbness in the upper thigh, so Dr. Larson checked the patient’s reflexes to see what nerve was hurting. Dr. Larson would ask the patient to move into certain positions that are shown below.

Flexing the foot upward was the hardest movement for Patient 1 to perform so the L4-L5 nerves were of concern. Patient 1’s MRI looked perfect in Dr. Larson’s words, so Dr. Larson wasn’t concerned that the nerve was pinched. To be sure, a CT scan was ordered. I found Patient 1’s scenario to be representative of the other patients' I observed. The majority of the patients were mostly in pain, but Dr. Larson explains that the pain is a result of an “insulted” nerve after surgery. Like Patient 1, CT scans were order for almost all the patients for reassurance.
Aside from going to clinic, I was able to watch an x-ray, an MRI, and a Kyphoplasty. A Kyphoplasty is a surgery used to treat compression fractures in the spine. People with osteoporosis are more likely to need this procedure. Dr. Larson uses a minimally invasive technique when he performs a Kyphoplasty. At the end of the Kyphoplasty I watched, Dr. Larson shaped the cement into a stick-figure man! Click Here to watch an animated video that illustrates the procedure.
Well, that is all for this week. After shadowing Dr. Larson in clinic, I realized how important it is to take care of your spine! Dr. Larson says twisting is one of the best things you can do to decompress the spine. Hold the following yoga pose for five minutes on each side! (Watch the video)
Half Lord of the Fishes Pose
Ciao,
Hannah




This comment has been removed by the author.
ReplyDeleteThis is very interesting, Hannah! I wondered, how do you get the patients to stay in the same position for their xray so your measurements are accurate. Or does that not matter? Thank you for your extremely well written updates.
ReplyDeleteThank you! I think the x-ray technicians try their best to align the patients in a standardized upright position to get these measurements. However, these standardized upright positions could also provide false information regarding the patients "actual" global spinal alignment. For example, if a patient comes in with a naturally hunched back and the x-ray tech asks the patient to straighten their back for their x-ray that x-ray won't actually depict that patient's true spinal parameter measurements, which could mislead the surgeon and so forth. I actually talked to one of the x-ray technicians about this and he said the position of a patient can change their lordosis, but they try the best they can.
DeleteWow! That is a lot of information! Have you noticed a trend in the data? Or did you have a hypothesis going in? Are you expecting lordosis to increase/decrease/no change as a result of these procedures?
ReplyDeleteYes I have seen more of a trend with the TLIF cages than with the PLIF cages. When I was using Surgimap to take these measurements, I found that a patient's global lordosis would increase from pre-op to post-op and then decrease again for the most recent measurement. In most cases, the segmental lordosis would stay the same from pre-op to post-op. However, I didn't see as big of a trend with the PLIF cage for global lordosis change. It really depended on the patient. But we will see after statistical analysis!
DeleteI originally thought that lordosis would increase after surgery, regardless of the cage type. However, Dr. Larson's hypothesis is that global and segmental lordosis stays the same from pre-op to post-op, regardless of the type of cage. I think that the global and segmental lordosis will increase for the TLIF cage, and I think that the global lordosis will remain the same for the PLIF cage and that the segmental lordosis will increase for the PLIF.