Week 6 & 7
Hi all,
This week, I have been working a lot on my research paper and reading more articles related to spinal fusion surgeries and lumbar lordosis. A week ago, I found a study from The National Center for Biotechnology Information called Improvement of Segmental Lordosis in Transforaminal Lumbar Interbody Fusion: A Comparison of Two Techniques. Since the results of this study were so interesting, I ended up sharing this article with Dr. Larson and it eventually shifted the design of our own research project.
Review of the Study
The aim of this research was to analyze the effects of a traditional transforaminal lumbar interbody fusion (TLIF) approach versus a cantilever TLIF (c-TLIF) approach on segmental lordosis, disk height, and segmental coronal alignment. (All I really care about is the segmental lordosis data.) The investigators conducted a retrospective review on a total of 101 patients who received a TLIF between the years of 2006 to 2011 by three different spine surgeons. Of the 101 patients, 40 received the c-TLIF approach with a kidney-shaped disk cage and 61 received the traditional TLIF approach with a straight disk cage. With the c-TLIF approach, the surgeon inserted the cantilever cage in the disk space behind the anterior longitudinal ligament (ALL), so the disk would be situated as far forward as possible. With the TLIF approach, the disk cage was also placed in the anterior region of the disk space but in a slanted direction. Neither of the disks had any inherent lordosis, meaning that the design of the graft would not curve the spine once placed in the space.
Image of the cantilever TLIF cage and TLIF cage

Rice, James W. "Fig. 1" The National Center for Biotechnology Information, Cara L. Sedney, Scott D. Daffner, Justin W. Arner, Sanford E. Emery, John C. France, vol. 6, no. 3, 2016, p. 230, The National Center for Biotechnology Information,2016, West Virginia. The Global Spine Journal, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4836934/
Image of the Anterior Longitudinal Ligament

Augusta University. "Anterior Longitudinal Ligament." Augusta University Health, http://www.augustahealth.org/spine/spine-glossary/spine-glossary-anterior-longitudinal-ligament-(all).
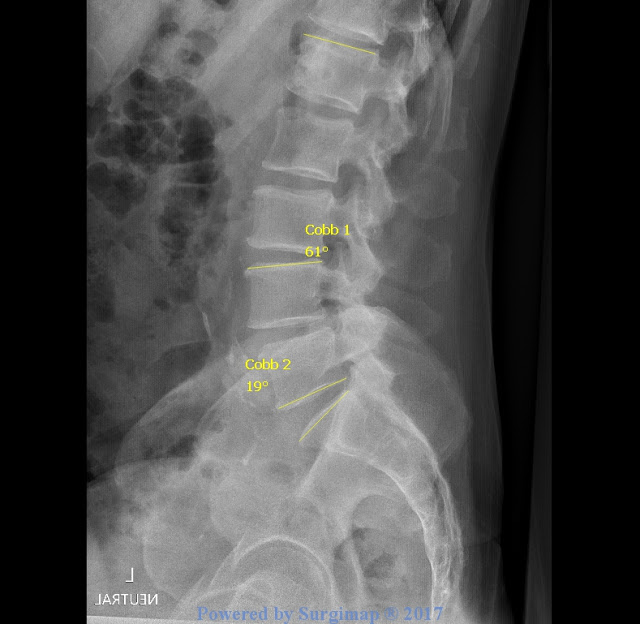
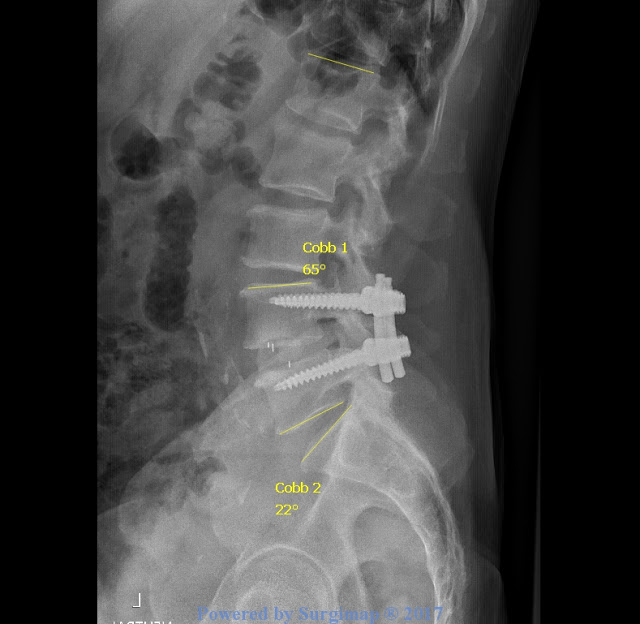
The investigators of the study used the Cobb method to take disk height, segmental coronal alignment, and segmental lordosis measurements from x-rays. (Again, segmental lordosis refers to the vertebrae of the spine where the spinal fusion was performed.) The investigators of the study took the measurements at the following times:
t0: x-rays taken on the day of surgery
t1: x-rays taken at patient's first postoperative follow-up (the average time for both the c-TLIF and TLIF group was six weeks)
t2: one year follow-up
t3: final follow-up (c-TLIF group: average final follow-up time was 26 months; TLIF group: average final follow-up time was 22 months)
The researchers subtracted preoperative measurements from every other following measurement. The mean change for each measurement was computed for both the c-TLIF and TLIF groups. Finally, statistical analysis was performed to compare the two groups' data by using a two-tailed t-test.
Results
c-TLIF Group
|
Mean ΔSegmental Lordosis (SL) from t0, t1, t2, t3 [°]
| |||
Mean Preoperative SL Value (°)
|
t0
|
t1 (mean= 6 weeks first follow-up)
|
t2
|
T3 (mean= 26 months final follow-up)
|
3.1
|
7.8
|
6.5
|
5.5
|
4.9
|
TLIF Group
|
Mean ΔSegmental Lordosis (SL) from t0, t1, t2, t3 [°]
| |||
Mean Preoperative SL Value (°)
|
t0
|
t1 (mean= 6 weeks first follow-up)
|
t2
|
t3
(mean=22 months)
|
5.6
|
4.0
|
1.8
|
0.4
|
0.1
|
After statistical analysis, the investigators found that patients in included in the c-TLIF category had segmental lordosis improved significantly (p<0.0001) compared to patients who received the straight TLIF cage.
So how does this relate to my research? Well, I sort of indicated in my last blog post that I would be looking at different cage types as a result of learning the implications of this Rice study. My advisor, Dr. Larson, believes that companies who specialize in spine instrumentation will be very interested to see if the type of cage used in a MIS TLIF affects lordosis. Yet, this study analyzes the effects of a traditional TLIF on segmental lordosis whereas mine will analyze the effects of a minimally invasive TLIF on both global and segmental lordosis. My research has never been done before, so the results of my research will be of great significance to spine surgeons since the preservation and restoration of lordosis is the optimal goal of many spine surgeries.
I intend to imitate this Rice study for my own research project by dividing my research subjects into groups based on the cage type used in the surgical procedure, compare patients' delta preoperative vs. postoperative measurements, and conduct a two-tailed t test to contrast the two groups' data.
That is all for this week! This week's yoga pose is Child's Pose! Click the link and try it out.
Until next time,
Hannah